1 Rehabilitation Engineering and Applied Research Laboratory, Georgia Institute of Technology, Atlanta, GA
2 Shepherd Center, Atlanta, GA
ABSTRACT
The objective of this study was to evaluate the biomechanical responses to tilt in persons with SCI. Changes in blood flow and loading at the ischial tuberosities (ITs) across different amounts of tilt were measured with Laser Doppler flowmetry and interface pressure. Pressure reduction at the IT was not present at 15°, but did occur with tilts to 30° and greater. Unlike pressure, blood flow increased with all tilts from an upright position. Only 4 of 11 participants had a considerable increase (≥10%) in blood flow at 30° tilt, whereas 9 participants did during maximum tilt (i.e., 45°-60°). Based on the results of this study, tilting for pressure reliefs as far as the seating system permits is recommended to maximize the potential for significant blood flow increases and pressure relief. The use of interim small tilts is also supported, as they also provide some benefit.
KEYWORDS
tilt-in-space, blood flow, interface pressure, wheelchair seating, pressure ulcers
BACKGROUND
The overall objective of our research is to improve the use of seated tilt to increase function, health and quality of life for people using power wheelchairs. Specifically, the goal of this project was to evaluate the biomechanical responses to seated full body tilt. This study also sought to develop initial guidelines for performing pressure relieving tilts.
Tilt systems are frequently prescribed to wheelchair users who are unable to independently reposition or perform pressure reliefs. However, little is known about the biomechanical effects of their use.
Pressure ulcers remain a major problem for many wheelchair users (1). In addition to having an obvious detrimental impact on health, pressure ulcers often disrupt the educational, vocational and community participation of wheelchair users, thus negatively affecting quality of life. Two factors, the magnitude of pressure and duration of loading, are the defining causes of pressure ulcers (2, 3). Clinically, these causative factors are addressed by the selection of an appropriate seating system, including a pressure distributing wheelchair cushion, and by the establishment of pressure relief schedules. Power wheelchair users who are unable to independently perform pressure reliefs are often prescribed powered tilt systems.
The Consortium for Spinal Cord Medicine suggested that tilt systems be utilized to perform weight shifts every 15-30 minutes for at least one minute (4). Although the required tilt angle to perform a pressure relief has not been defined, research has shown that interface pressure decreases as the tilt angle increases. Therefore, recommendations in the literature and clinic vary from 30° to 65°, with an emphasis on tilting “all the way back”.
In this study, Laser Doppler flowmetry and interface pressure measurement were employed to measure the increase in blood flow and decrease in loading with increased tilt angle on participants with SCI. Two hypotheses were tested:
H1. The minimum tilt position required to increase blood flow was less than 45°.
H2. There was a significant decrease in loading at the minimum tilt required for increased blood flow.
METHODOLOGY
This study was approved by the local institutional review boards and participants signed informed consent prior to participation. Eleven participants with SCI who used power tilt-in-space wheelchairs were recruited to participate. Measurements of superficial blood flow were done using the PeriFlux 5010 LDPM (Laser Doppler Perfusion Monitor) and a custom probe (Figure 1, LEFT). A custom sensor from FSA (Vista Medical, Winnipeg, Manitoba) was utilized to monitor the localized loading surrounding the LDFM probe (Figure 1, RIGHT).
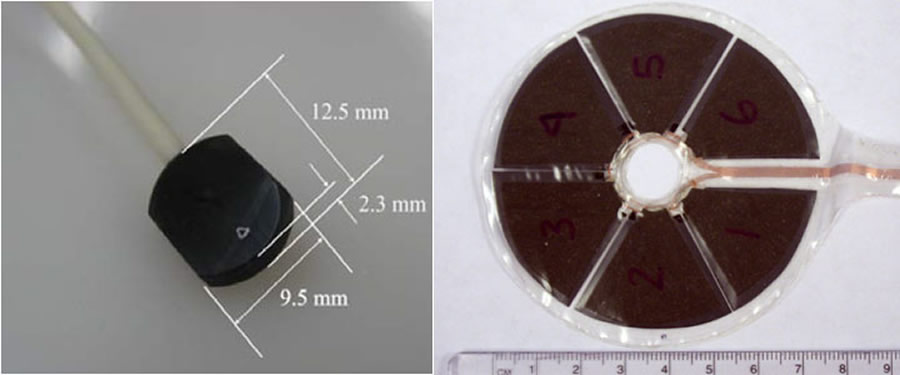 Figure 1. (Left) Laser Doppler flowmetry probe (Right) Interface pressure sensor
Figure 1. (Left) Laser Doppler flowmetry probe (Right) Interface pressure sensorInitially, participants donned a pair of stretchy boxer shorts and were lifted with an overhead lift and a Guldmann net to provide access to the ischial region while maintaining a relatively upright, seated posture. With the subject lifted, the interface pressure sensor and LDPM probe were attached to the skin directly superficial to the apex of the ischial tuberosity.
Three randomized trials of the following, alternating sequences were performed in the participants’ personal wheelchairs: Upright (or minimum tilt position) to 15°, Upright to 30°, Upright to 45°, and Upright to maximum tilt. All seated positions were held for 2 minutes and trials were separated by 5 minutes of unloaded sitting (lifted in the Guldmann net). LDFM was sampled at 32 Hz and the interface pressure sensor was sampled at 1 Hz throughout the duration of the above testing.
All data analysis was performed with Matlab R2008a (Mathworks Inc, Natick, MA). Average blood flow was calculated as the average reading over the final minute at each position. Blood flow at each tilted position was normalized by blood flow at the preceding upright position. Maximum pressures across all sensels were analyzed. All statistical comparisons were computed with paired, one sided t-tests.
RESULTS
Subjects included 9 men and 2 women with mean (SD) height 1.79m (0.04m) and weight 80kg (14kg). Seven subjects were African American, 3 were white, and 1 identified as biracial. Research participants had been using a wheelchair for a mean (SD) of 9.4 (5.7) years, with a minimum of 9 months and a maximum of 18 years.
Wheelchair configurations were not modified for this study. The upright position in all chairs was less than or equal to 5° (mean (SD) = 2.1° (1.8°)). Seat to back angles ranged from 90° – 110°, with a mean (SD) of 101° (6°).
Tilt Position |
Max Pressure (mmHg) |
Mean Pressure (mmHg) |
Mean Normalized Blood Flow |
Upright |
91 (32) |
74 (27) |
n/a |
15° |
87 (30) NS |
71 (25) ** |
1.08 (0.19) * |
30° |
77 (28) ** |
62 (24) ** |
1.24 (0.48), * |
45° |
63 (25) ** |
50 (21) ** |
1.84 (1.84), * |
55° |
68 (27) ** |
53 (23) ** |
3.34 (5.09), * |
Peak pressures in the region surrounding the ischial tuberosity in upright sitting varied across participants from 27 to 176 mmHg (Table 1). Although there was no decrease in pressure at 15°, there were significant decreases at all other tilt positions.
We used multivariate linear regression to create a model to predict the maximum pressure based on tilt angle with R2 = 88.1 (Equation 1).
|
35° Tilt |
45° Tilt |
55° Tilt |
|||
Pressure in Upright (mmHg) |
mmHg |
% |
mmHg |
% |
mmHg |
% |
50 |
41 |
82 |
34 |
67 |
27 |
53 |
100 |
81 |
81 |
74 |
74 |
66 |
66 |
150 |
122 |
81 |
115 |
76 |
107 |
72 |
This model is individualized based on the initial, upright pressure. All coefficients in the model were significantly different than zero (p<0.001). Because interpretation of a multivariate model can be confusing, Table 2 presents some examples of what the model would mean at a 35°, 45° and 55° of tilt for people with different initial loads.
Blood flow results were highly varied across subjects (Table 1). For instance, only five subjects appear to have blood flow that increases monotonically with tilt angle. Two subjects had limited or no increase in flow with tilts up to 45° but had considerable blood flow increases at maximum tilt. On average, all tilt positions resulted in a significant increase in blood flow. Although it was statistically significant, the increase in blood flow at 15° of tilt was only 8% and was highly variable across subjects (SD = 19%) (Table 1). Nine of the eleven participants showed a considerable increase in blood flow at the terminal tilt position available on their wheelchair. On the other hand, only 4 of 11 participants had an increase in blood flow of ≥ 10% at 30% tilt.
The results supported our first hypotheses, that the minimum tilt position to increase blood flow (i.e., 15⁰), was less than 45⁰. However, the second hypothesis, that there was a significant decrease in loading at the minimum tilt required for increased blood flow was not supported, as pressure did not significantly decrease at 15⁰.
DISCUSSION
This study produced a number of interesting results: 1) A significant increase in blood flow at 15° of tilt was not accompanied by a drop in pressure, suggesting a different mechanism for the increase in blood flow. 2) Changes in blood flow and pressure are highly individualistic. 3) Terminal tilts (45°-55°) produced the largest changes in pressure and blood flow across the most subjects.
Based on these results, we can offer some preliminary guidelines for pressure relieving tilts. First, we would recommend tilting for pressure reliefs as far as the seating system permits. Additionally, until we understand more, we should not neglect the potential impact of small tilts. As described previously, the increase in blood flow due to small tilts cannot be attributed entirely to a decrease in pressure. Therefore, it is unknown whether these small tilts might provide a different benefit to the body from the weight shifts at a full tilt. As described in earlier research (5), small tilts also have many functional benefits over large tilts and might be a helpful option in between large tilts.
These preliminary guidelines for a pressure relieving tilt must be interpreted cautiously. With only 11 participants, most of whom were sitting on a Roho air inflation cushion, it is unclear whether the results will generalize to a larger population and other wheelchair cushions. For example, in Stockton and Rithalia’s blood flow work, they found that forward leans on a Roho resulted in a smaller pressure reduction and blood flow increase compared to a gel cushion, suggesting that the effect of tilt on pressure reduction and blood flow might differ according to cushion type (6). However, the recommendation put forth in this study does err on the side of caution. Future research will hopefully be able to individualize the guidelines based on personal characteristics.
REFERENCES
- Salzberg CA, Byrne DW, Cayten CG, van Niewerburgh P, Murphy JG, Viehbeck M. A new pressure ulcer risk assessment scale for individuals with spinal cord injury. American journal of physical medicine & rehabilitation / Association of Academic Physiatrists1996 Mar-Apr;75(2):96-104.
- Kosiak M. Etiology and pathology of ischemic ulcers. Arch Phys Med Rehabil1959 Feb;40(2):62-9.
- Reswick J, Rogers J. Experience at Rancho Los Amigos Hospital with devices and techniques to prevent pressure sores. In: Kennedy CaS, editor. Bedsore Biomechanics. Baltimore: University Park Press; 1976. p. 301-10.
- Pressure Ulcer Prevention and Treatment Following Spinal Cord Injury: A Clinical Practice Guideline for Health-Care Professionals. In: America PVo, editor.: Consortium for Spinal Cord Medicine; 2000.
- Sonenblum SE, Sprigle S, Maurer C. Use of Powered Tilt Systems in Everyday Life. Disability and Rehabilitation: Assistive Technology2009;4(1):24-30.
- Stockton L, Rithalia S. Is dynamic seating a modality worth considering in the prevention of pressure ulcers? Journal of tissue viability2007 Feb;17(1):15-21.
ACKNOWLEDGEMENTS
Funding was provided by NIDRR through the RERC on Wheeled Mobility (H133E080003).
AUTHOR CONTACT INFO
Sharon Eve Sonenblum
490 10th Street NW
Atlanta, GA 30318
404-385-0633
sharon.sonenblum@coa.gatech.edu